Drooling in Parkinson’s Disease
Sialorrhea or drooling is a major unmet need that may affect people with Parkinson’s (PwP) over the course of their disease. The average person swallows about 1,000 times a day - and for most of us we don’t even know we are doing this. Drooling in PwP occurs when there is excessive saliva in the mouth which leaks out because people with Parkinson’s may subconsciously not be swallowing frequently enough. This is important to recognize because not only is drooling uncomfortable and embarrassing but excessive saliva can also occur in the throat and lead to aspiration.
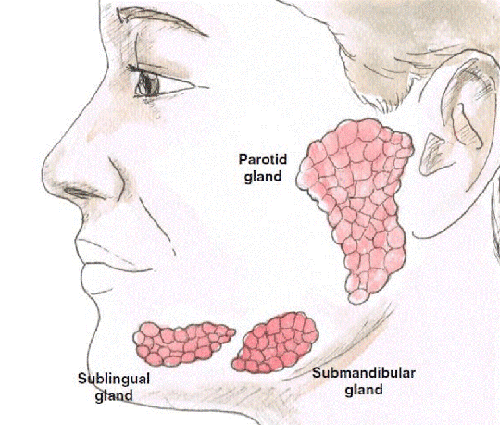
There are three major salivary glands: in front of the ear lobe (parotid); under the jaw (submandibular); and under the tongue (sublingual). These are the glands that create the saliva which plays an important role for the body including but not limited to:
- wetting and softening the food to help start digestion;
- cleaning and lubricating inside the mouth;
- stimulating taste buds which is particularly important for people with Parkinson’s who may have lost their sense of smell; and
- aiding in swallowing.
Why does drooling occur?
Drooling in Parkinson’s is not because of excessive saliva production but instead because of swallowing issues or decreased swallowing due to a weakening of muscles in the throat. In addition to the decreased swallowing or weakening of muscles, PwP may have poor posture or experience excessive daytime sleepiness. Because of these issues PwP may sit with their neck in a forward position, with their mouth open, without even realizing it which leads to gravity causing saliva to pool in the mouth and overflow.
Over the course of the disease, drooling occurs in 30-70% of PwP and can be severe in up to 10%. Drooling can also cause impairment in speech which may negatively impact social interactions. Because of this, it’s recommended that PwP start working with a speech language therapists/pathologists(SALT/SLPs) who specialize in Parkinson’s early in their diagnosis. Even if the person has no symptoms of speech impairment or swallowing challenges initially, if they work with a SALT/SLP from the start, this expert can help them work on swallowing technique and strengthen throat muscles, possibly helping to delay, minimize, or stop drooling from ever becoming an issue.
Because of the postural challenges, it’s recommended that PwP also start working with a trained physical or occupational therapist who can work with the person to improve posture. Proper posture can aide in swallowing, by just giving cues to keep the head from tilting forward. . The idea is that it’s best to train the body ahead of time to prevent challenges, rather than to just treat once they become an issue.
Excessive saliva in the mouth can also lead to other issues that should be addressed such as dental issues, pneumonia due to aspiration, and psychosocial challenges. It’s recommended that you speak to your dentist about Parkinson’s and discuss a dental care plan that works for you. You may also wish to use an electric toothbrush to aid in dental care since limited fine motor skills may not allow for a thorough cleaning.
If drooling keeps a PwP or care partner from wanting to socialize this could increase depression and anxiety. If this is something you are experiencing, it’s recommended that you ask your doctor for a recommendation to speak to a social worker/therapists who can help navigate some of these issues as individuals and as a couple.
Are certain PwP at higher risk for experiencing drooling?
Risk factors for drooling include older age, male gender, longer disease duration, more severe disease, occurrence of hallucinations and dementia, swallowing and speech difficulty, low blood pressure on standing leading to dizziness, and certain medications. While the majority of these factors cannot be changed to reduce drooling, there are things health professionals and PwPs can do to address this symptom.
How can drooling be managed?
The first step in managing drooling is to speak to your movement disorder doctor. Certain medications used for memory issues like rivastigmine and medications for hallucinations like quetiapine and clozapine can cause drooling. In some cases, these medications can be changed to ones that do not cause drooling. Your doctor is the best one to work with you on evaluating your medications to see if an adjustment in your treatment plan makes sense.
Your doctor will then look at medical management of the motor symptoms of PD including bradykinesia, rigidity and OFF time. He/She may have you evaluated and managed by a SALT/SLP to improve mouth muscle coordination and swallowing if you are not already seeing someone. If the PwP isn’t already seeing a physical therapist, the doctor may have the PwP undergo evaluation and training for improved head and body posture, including the use of neck support collars, education regarding keeping the mouth closed, reminders for frequent swallowing such as chewing gum or sucking on hard candy might also be helpful. With more severe drooling, the use of suction machines may be considered.
The most common medications used for drooling are anticholinergics. Since one of the most common side effects of these medications is memory impairment, they should be used cautiously in PwP who may already experience these issues. It’s important to note that none of these treatments are FDA approved, but they are things PwP can discuss with their doctors and should not be done without medical supervision. Glycopyrrolate tablets can also be helpful for drooling. Some doctors may use atropine eye drops or ipratropium bromide nasal spray used under the tongue which might be helpful but should only be administered with medical supervision.
Botulinum toxin injections in the parotid and submandibular salivary glands are increasingly being used to treat drooling. Rimabotulinumtoxin B (Myobloc) and incobotuliumtoxin A (Xeomin) are approved by the FDA and EMA for the treatment of drooling in the US and Europe. Incobotuliumtoxin A (Xeomin) is the only approved botox treatment in Europe. Rimabotulinumtoxin B is the most commonly used toxin for drooling. Patients usually receive 2-6 injections with small needles in front of the ear and below the jaw. These injections are performed through the skin and not through the mouth. These injections reduce the production of saliva for 8-12 weeks and consequently reduce drooling. The injections are repeated approximately every 3 months. The most common side effects include pain at the site of the injection, dry mouth and rarely swallowing difficulty. Due to reduced saliva production, there may be increased risk of dental decay or cavities.
In rare cases, radiation to the salivary glands and surgical intervention such as tying the salivary duct or removal of the salivary glands has been attempted but is not usually recommended.
In summary, drooling in PwP occurs due to swallowing difficulties. Drooling can lead to social isolation and reduced quality of life for both the person with Parkinson’s and the care partner. It occurs with advancing disease and can be a challenge to manage but it’s important to know that health professionals can help and that different members of the health care team can play a role, including the physical and/or occupational therapist and speech language pathologist. Ideal management of the motor symptoms of PD would include consultation with a movement disorder doctor to ensure the medication dosage is optimal and to explore best treatment options if experiencing drooling.
In addition to this, working on improved posture with a physical therapist can help train the PwP on proper sitting techniques and the team can also help educate on cues to remind the PwP to swallow and tilt his/her head back. Consultation with a SLP/SALT who specializes in Parkinson’s is recommended for training on swallowing and exercises to strengthen throat muscles. Oral medications are often limited in the management of drooling due to side effects. Botulinum toxin injections into the parotid and submandibular glands may also be considered.
Take away tips for addressing drooling in Parkinson’s
1. Consult with your movement disorder doctor about your concerns, challenges, and discuss treatment options, and possible medication adjustment
2. Ask for a recommendation to see a qualified physical or occupational therapist who has experience with Parkinson’s
3. Ask for a recommendation to see a qualified SLP/SALT who has experience with Parkinson’s
4. Keep hard candies on hand to suck on, as this will help remind you to swallow. Best to make them sugar free candies to decrease risk of cavities.
5. Drink more fluids, ideally water, to help “wash” down the saliva. This is also recommended since water can help lessen the chance of constipation.
It’s important to remember that if you are experiencing drooling that you speak to your doctor. You are not alone and there are options for treating this symptom.
Resources:
Blog post by Frank Church, PhD, WPC 2019 Program Committee member:
https://journeywithparkinsons.com/2019/01/22/parkinsons-and-sialorrhea-drooling-or-excessive-salivation/
Blog post by Maria de Leon, MD, WPC 2022 Parkinson Advocates Committee member:
https://defeatparkinsons.com/2014/07/31/10-tips-for-managing-drooling-in-parkinsons-by-dr-de-leon/
Parkinson’s Foundation’s Fitness Friday video on posture: https://youtu.be/WRyPQO_u_qE
Rajesh Pahwa, MD is a member of the World Parkinson Coalition Board of Directors. He has spoken at past World Parkinson Congresses and Chaired the WPC Fundraising Committee for WPC 2016 and WPC 2019. He is currently the Laverne & Joyce Rider Professor of Neurology, Chief of the Parkinson and Movement Disorder Division and Director of the Parkinson’s Foundation Center of Excellence at University of Kansas Medical Center in Kansas, USA.
Ideas and opinions expressed in this post reflect that of the authors solely. They do not reflect the opinions or positions of the World Parkinson Coalition®